
This procedure is indicated only when the femoral head has good cartilage and the acetabulum is absent or has inadequate cartilage for other acetabular procedures to help. This condition is seen in long standing untreated spontaneous hip dislocation. A few small case series have shown good results that can last for a long time. Reinhold Ganz popularized it recently. It restores near normal hip morphology and mechanics and makes future conversion to a total hip easy. Other requisites for this procedure to be successful are
- Round femoral head that can fit into the new acetabulum
- Adequate capsular tissue available for interposition
- Strong hip abductors that will avoid shear stress on the joint.
The initial capsulotomy has to be circumferential all around the acetabulum. The capsular flaps are designed to cover the head well all around. The new acetabulum is reamed at the hip center. It can be augmented with the bone from femoral shortening. The femoral shaft is shortened to bring the femoral head down to the hip center. The femoral head can be made round and smaller if needed. The capsule is placed on the head and its flap sutured to create a round head covered with capsule. The capsule covered head is reduced into the new acetabulum and immobilized there for 2 weeks in a hip spica cast. The cast can be opened in the front after 2 weeks to allow hip flexion under the supervision of a physical therapist. Once the capsule adheres to the cancellous bone of the new acetabulum, hip abductors have to be strengthened to decrease the shear force on the capsule generated by the Trendelenberg lurch from unsupported weight bearing.

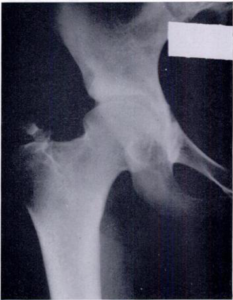
Dislocated right femoral head with very shallow acetabulum. Red line outlines the stretched out capsule.
Reduced right femoral head several years after reaming an acetabulum and capsular interposition