
Impingement in one region of the hip can produce a lever effect on the femoral neck and subluxatory stress on the femoral head in the region that is on the opposite side of the hip.
Anterior impingent – Posterior instability
The premature contact between the femoral head-neck junction and acetabulum anteriorly from decreased internal rotation in 90 degrees of flexion (FIR) caused by anterior cam, femoral and acetabular retroversion causes anterior impingement. Attempts to get more internally rotation of the hip produce subluxatory stress on the head posteriorly. The normal hip capsule prevents such subluxation, but the posterior forces can produce shear stresses on the posterior acetabular cartilage and labrum by the supra foveal part of the femoral head called Contre-coup damage. Suprafoveal damage in SCFE and cysts in the head in that region are probably from this mechanism.
Significant trauma can tear the posterior hip capsule and produce acute posterior dislocation – Most posteriorly dislocated hips have risk factors for anterior impingement and decreased FIR. Though recurrent dislocation is not common, chronic discomfort in these hips can be from persistent anterior impingement and posterior instability. We recommend assessment of FIR and correction of anterior impingement in these hips. Even the posterior dysplasia may need correction and posterior dysplasia may indicate open reduction and internal fixation of even a small posterior wall fracture.
Recurrent dislocation of total hips is almost always from anterior impingement of malpositioned femur and or acetabulum. The definitive treatment is revision of the component position.
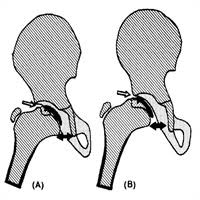
Hinged abduction
Lateral impingement of the hip from an irreducible lateral part of the head in hip abduction causes medial space widening or subluxation see on radiographs obtained in hip abduction. Bilobed heads develop from pressure of the acetabular rim on the subluxated femoral head. Treatment options for hinged abduction are
 https://italcultur.com/incompatibilita-sessuale-come-salvare-una/
https://italcultur.com/incompatibilita-sessuale-come-salvare-una/
- Valgus osteotomy of the femur to move the lateral impingement point laterally to increase abduction before the hip impinges. This can bring the fovea up against the weight bearing sourcil.
- Open reduction of the lateral head under the acetabular roof expecting remodeling of the bump and the acetabulum against each other. This is likely to work in children with open triradiate cartilage resulting in aspherical congruity.
- Shelf augmentation of the lateral acetabulum to cover the lateral head that decreases the lateral bump against the new acetabulum.
- Head reduction osteotomy to make the head spherical and open reduction of the smaller round head into the acetabulum. Instability of the smaller head from the often dysplastic acetabulum and capsule is divided for the surgical approach requires a concomitant acetabular osteotomy.