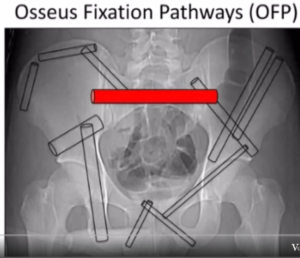
There are seven straight corridors or tunnels in the pelvic bone for safe insertion of implants.
- Iliosacral tunnel through S1 – Most commonly used for screw placement. Most affected by sacral dysmorphism. Careful evaluation of xray and CT scan are important to identify safe screw path. Intraop verification requires interpretation of the anatomy from the inlet, outlet, and lateral views and palpation of the drill hole like probing the pedicle. None of the xray views show the sacral ala directly. Lateral view shows the iliac condensation that correlates with the alar slope in the normal pelvis. Contents of the spinal canal, S1 root in its foramen, and L5 root over the sacral ala are at risk from the drill and the screw.
- Iliosacral tunnel through S2 – Less variable and less risky to neural elements allowing safe insertion of one screw trans-sacrally from one SI joint to the other based on Outlet, inlet, and lateral views. S1 and S2 nerve roots in their foramena, cauda equina in the spinal canal, and median sacral artery in the front are at risk.
- Supra acetabular tunnel – a large column of bone just above the acetabulum and greater sciatic notch extending from the antero-inferior iliac spine (AIIS) to the poster-superior iliac spine (PSIS). An obturator outlet view (Tepee view) shows the axial view of this tunnel and the iliac oblique view shows the length and makes certain that the screw is above the greater sciatic notch. This space can accept one or two very large screws used for pelvic fracture fixation from the front or the back and lumbopelvic fixation from the back. The screw from the back can be inserted into S2 ala and advanced across the SI joint into the supraacetabular tunnel. (S2AI screw) This position makes the screw head less prominent in the back and lines it up with lumbar pedicle screws obviating the need for rod bending or use of a connector.
- Anterior column of the acetabulum – Extends from the supraacetabular bone laterally through the superior pubic ramus to the pubic tubercle. Obturator oblique view shows its length and extra-articular placement of implants. Inlet view shows anterior or posterior deviation of the drill. The concavity of the superior pubic ramus medial to the ilio-pectineal eminence is not easily seen and femoral artery and vein are very close to the superior surface of pubic ramus and obturator nerve and vessel are close on its inferior side at this level. Screws can be placed from lateral to medial or medial to lateral.
- Posterior column of the acetabulum – Extends from the pelvic brim to the ischial tuberosity lying posterior to the acetabulum and anterior to the greater and lesser sciatic notches. Screws can be placed antegrade through the iliac fossa or retrograde from the ischial tuberosity. AP and iliac oblique views are adequate and an oscillating drill tipped guide wire is helpful to feel bone better.
- Iliac crest – The bone below the crest is thick and can take interfragmentary screw fixation of iliac fractures. The crest is thickest over the gluteal pillar allowing insertion of two to three pins for external fixation.
- Inferior ramus – Ischial tuberosity to the pubis along the inferior ramus is rarely used for implant placement though screws from the anterior plate on the pubis and posterior plates over the ischium do extend into the inferior ramus to a variable length.