
Triple Innominate & PeriAcetabular Osteotomies
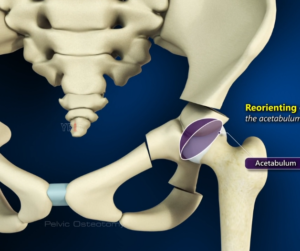
Acetabular deficiency in older children or mal-orientation of the acetabulum at any age are best treated by freeing the acetabulum from rest of the pelvis and redirecting it to increase coverage of the femoral head and optimally orienting it to rest of the pelvis.
Triple innominate osteotomy involves complete division of pubis, ischium and ilium away from the growth plates and hence can be performed at any age. The Tonnis 2 triple osteotomy will give an acetabular fragment that is free from all tethers and as mobile as a periacetabular osteotomy. Triple osteotomy has the disadvantages of disrupting the pelvic ring and healing issues with bigger corrections when the gap gets bigger.
Periacetabular Osteotomy (PAO) is the most desirable pelvic osteotomy when triradiate cartilage growth is not considered significant anymore (after 8 years of age). The osteotomy involves a complete pubic osteotomy, partial ischial and iliac cuts freeing the acetabulum while leaving the posterior half of the posterior column intact. The fragment retains adequate blood supply and healing potential even with large corrections. PAO is also the most difficult procedure to learn with a steep learning curve and serious potential complications.

Both osteotomies can be performed through a single anterior incision for all the cuts or single lateral approach when combined with surgical dislocation or femoral osteotomy.
Sequence of femur and acetabular procedures
Whenever both femoral and acetabular osteotomies are indicated, approach to the femur can be used for the ischial osteotomy even if the other cuts will be performed through a separate anterior approach.
Periacetabular osteotomy postop protocol
POD #1
PT – Mobilize with toe touch weight bearing, No other restrictions unless surgical dislocation was performed and instability of the hip joint is a concern.
Reinforce dressings as needed.
Teds for 10 days
SCDs while in house.
Aspirin 325 mg q day for 14 days
Pelvis AP x ray. Consider adjustment of acetabular orientation if needed in the first week.
POD #2
Remove epidural, catheter, and drain.
Reinforce dressings as needed. Do not change them.
Hip motion as tolerated.
Ambulate 100 ft twice a day.
Occupational therapy to evaluate and treat for ADLs.
Discharge planning
POD #10
Pelvis AP Xray.
Remove dressings and sutures.
Stationary cycle at low resistance for 20 minutes twice a day.
POD #30
Pelvis AP x-ray.
Increase weight-bearing based on healing of the osteotomy.
Increase the resistance on the cycle.
POD # 60
Pelvis AP x-ray.
Increase weight-bearing based on healing of the osteotomy.
Abductor strengthening.
Physical therapy
POD # 90
Resume normal activities.